Introduction. Bladder Leiomyoma is a rare benign nonepithelial lesion which represents 0.04–0.5% of bladder tumors found in females between the age 40 to 50 [1]. The incidence of leiomyoma in pregnancy is rare and only four cases of bladder leiomyoma during pregnancy have been reported previously. To our knowledge, this case is the fifth case to be reported.
It origins from the smooth muscle bundles and therefore it can be found at any organ with this kind of tissue [1]. In the urinary system, the most frequent localizations are kidney and bladder. In the bladder, these lesions could be located at any level intramurally [2].
An occurrence of this tumor, it is believed to be related to an endocrine alteration [3]. Surgery is the standard treatment and the surgical approach depends on tumor size and localization at the bladder wall. Prognosis is good due to the benign behavior of these lesions [1].We present the case of a subserosal bladder leiomyoma presenting as malignant ovarian tumor in a 29-year primigravid.
Case report. 29 years old healthy lady, primigravida at 13weeks of pregnancy, presented with painless right-sided abdominal mass since March 2016. Initially patient sought treatment at the private clinic who subsequently referred the patient to HUSM O&G team as transabdominal ultrasound revealed suspicious right pelvic mass. The transabdominal and transvaginal scan was done and revealed, a huge solid tumor which lies adjacent to the uterus. The mass measuring 16.2x17.7 cm lies more on right iliac fossa and suprapubic region, extending up till the epigastric. Uterus 15x10cm with intrauterine pregnancy. Otherwise no hydronephrosis, no ascites, and liver are homogenous. Blood investigations is non-significant and tumor marker was shown CA 125:18, CEA:0.9, LDH:319, and Beta HCG: <0.1
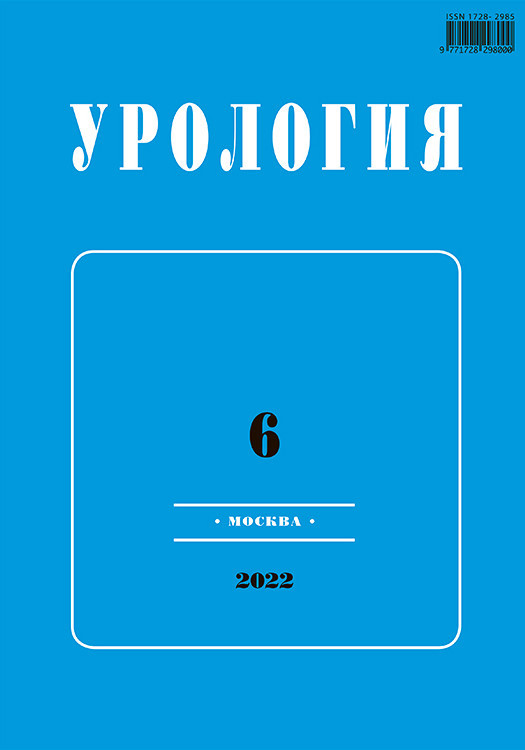
The patient was subsequently arranged for contrast-enhanced CT abdomen and pelvis and it showed a large heterogenous enhancing mass in the right hemipelvis extending to the intrabdominal cavity till the level of L4 vertebral body. It measures approximately 9.6 x13.2x14.5cm (AP X W X CC).The mass shows heterogenous enhancement post contrast with an area of nonenhancement suggestive of necrosis with no within calcification. A fat plane with the urinary bladder and uterus also preserved. No lung, liver or bone lesions seen. Impression, large pelvic mass likely malignant ovarian tumor (Fig. 1–4).

The patient was prepared elective laparotomy & right salphingo-oophorectomy & omentectomy (Fig. 5–7). The laparotomy revealed the mass arise from the bladder hence the urology team was called upon intraoperatively. The flexible cystoscopy was done and there was no intraluminal extension of the tumour from the examination. Intraoperatively, there were benign looking huge bladder tumor arising from dome of bladder (not involving bladder mucosa) measuring 20x20cm.Tumour noted to be highly vascularised. Gravid uterus and both the ovaries are normal looking.
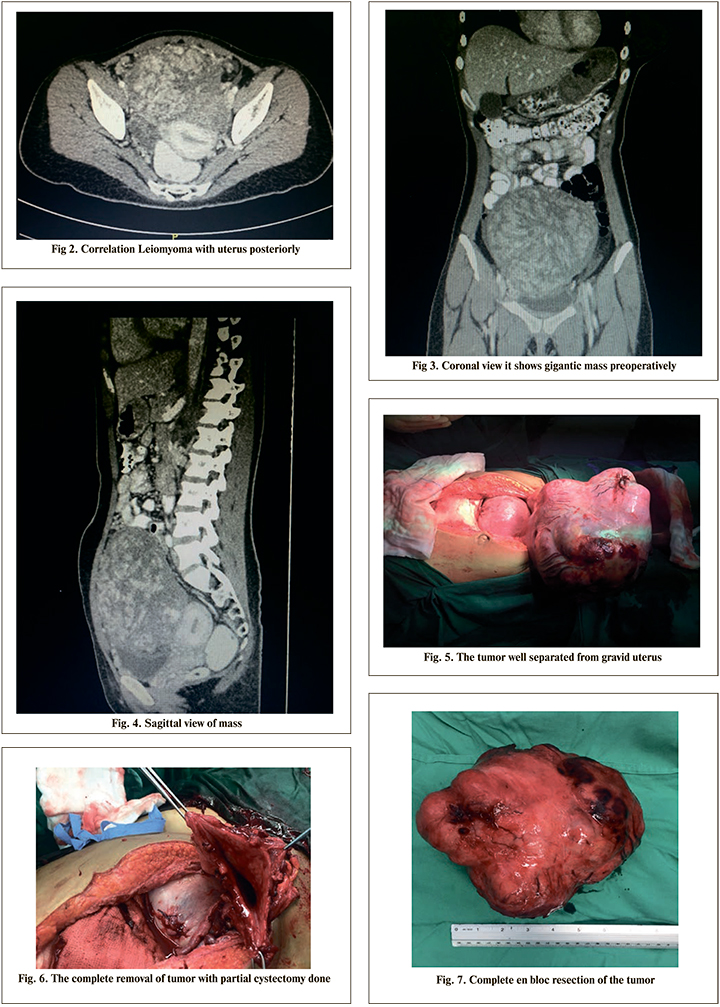
Complete resection of tumor and partial cystectomy was done with bladder repair. Suprapubic catheter size 16Fr was inserted. Post operative was uneventful and patient recovered well. Two weeks post procedure both Foley’s catheter and suprapubic catheter successfully removed, and patient was discharged home.
HPE results revealed well-circumscribed mass composed of interlacing bundles of smooth muscle fibers. The mildly pleomorphic tumor cells have oval to elongated vesicular nuclei with inconspicuous nucleoli. They also have long slender eosinophilic cytoplasmic processes. No mitosis is seen. Impression, bladder wall tumor, leiomyoma.
Discussion
The bladder leiomyoma is a benign mesenchymal neoplasm and it represents 0.5% of all bladder tumor, with only 250 cases was reported worldwide to date [4]. Although it is believed the incidence are equally distributed among men and women, however recent literature shows there is predominant in women from third until the sixth decades of age [5]. The bladder leiomyoma can be divided into endocervical, intramural and extravesical form [1, 5]. The endocervical form reported to account for 63%, the extravesical is 30% and intramural 7%.The symptoms can vary from asymptomatic usually for the intramural and extravesical form and its also usually be incidentally found [6]. Whereby the endovesical form usually presented as obstructive and irritative voiding symptoms and hematuria [2]. Goluboff et al reviewed all reported cases of leiomyoma of the bladder in the English literature since 1970 [5]. They indicated that obstructive voiding symptoms were the most common presenting patient complaint (49%). Of the remaining patients, 38% presented with irritative symptoms, 11% with hematuria, and 19% were asymptomatic. Knoll et al indicated that irritative voiding symptoms were the most frequent presenting symptom [6]. Like for our case, the patient presented with huge abdominal mass and discomfort due to the mass effect of the tumor. The mobile, nontender and smooth lesion of the bladder or pelvis frequently revealed during bimanual examination.
Regards to the imaging modality, ultrasonography can be one of the best non-invasive modality for earlier approach to the bladder leiomyoma, it could reveal smooth-walled solid lesion with homogenous echogenicity and determine the endovesical, intramural or extravesical nature of the lesion [7]. The relation between adjacent organ structure also could be shown using transvaginal ultrasound as been reported by Fernandez and Mayoyo [8]. Excretory urography may show irregular filling defects of the bladder, with or without ureter obstruction. Hydronephrosis may exist due to increased intravesical pressure caused by bladder outlet obstruction or direct compression of a ureter orifice. Despite all imaging, the CT scan is an accurate tool for localization and detection by presenting as homogenous mass with heterogenous or homogenous enhancement [9]. The magnetic resonance imaging (MRI) better demonstrates contrast among other structures tumor, bladder muscle, and extravesical fat [9].
Compared to CT, magnetic resonance imaging (MRI) better demonstrates contrast among urine, tumor, bladder muscle, and extravesical fat [10]. However, MRI still cannot be relied on unfailingly to differentiate leiomyoma from leiomyosarcoma, because both may enhance after contrast media administration [11]. Thus, this benign lesion should be removed completely and confirmed by pathologic examination.
The treatment of leiomyoma is determined mainly by its size and location [12]. The patient who does not have symptoms can be conservatively treated with periodic monitoring. As it was reported by Goluboff et al, 62% was treated with open resection and 30% by transurethral resection. Of the 62% who underwent open resection for large endovesical tumors, extravesical tumors, or intramural lesions, none required a second procedure [5]. They are managed with enucleation or partial cystectomy. Like in our patient, we done the surgical intervention in the current period of pregnancy because the tumor was suspected to be malignant, hence the immediate intervention need to be done. It has also been reported that leiomyoma of the bladder has been safely and effectively resected laparoscopically [13]. The prognosis of this tumor is excellent and no malignant transformation is reported. To date, our patient has good outcome and she had no problem with her pregnancy.
In summary, we reported a case of large bladder leiomyoma and the complete resection was performed in this patient because malignancy can’t be rule out after complete imaging studies. Careful physical examination and ultrasound may discover it ocassionally and the prognosis is excellent.